When the virus that causes mpox jumped onto the international stage in 2022, countries around the world, including the United States, turned to vaccines targeting the closely related smallpox virus to curb its spread. Yet it wasn’t until 2024 that Africa, the continent where the virus emerged and first began spreading among people, received its first doses.
On September 13, the World Health Organization authorized a smallpox vaccine called Jynneos, made by Danish pharmaceutical company Bavarian Nordic, for use to tackle growing mpox outbreaks — an administrative move meant to speed distribution. Nigeria had received 10,000 doses on August 27 as part of a donation from the United States, and another roughly 99,000 shots arrived in the Democratic Republic of Congo on September 5. But other countries in Africa are still waiting, and millions more doses are needed to address growing mpox outbreaks in Central Africa, even as researchers rush to learn more about the virus and its spread.
Congo is at the center of the surge in mpox (formerly known as monkeypox) cases that sparked a new public health emergency declaration from the WHO (SN: 8/14/24). The sometimes deadly disease has long been a problem in the region, causing symptoms including fever, muscle aches and a hallmark rash that looks like pimples or blisters.
Since the first mpox case in 1970, most cases have popped up sporadically in young children, usually after exposure to wild animals such as rodents or primates infected with the virus, and sometimes sparked small outbreaks (SN: 6/25/22). But Congo has had a steady rise in cases over the last decade, driven by viruses belonging to a subgroup called clade I. Behind the latest health emergency are clade I versions spreading person-to-person in a growing number of countries, including through sexual networks.
“As scientists, we’re not surprised [that this is happening] because we’ve been ringing the bell for some time,” says Jean Nachega, an epidemiologist at the University of Pittsburgh. “But looks like not too many people were listening.” Scientists are trying to catch up on missed decades of vaccine, drug and diagnostic research for a long-neglected disease.
The first mpox-related public health emergency that hit the Americas and Europe hard in 2022 — caused by viruses from a different branch of the family tree called clade II — ultimately faded and officially came to an end in May 2023 after global cases declined. But few resources made it to Africa, and virus’ spread there wasn’t resolved. Now, a new group called clade Ib has emerged in Congo that appears more able to easily spread among people.
“Viruses thrive on opportunity,” says Boghuma Titanji, an infectious diseases physician at Emory University School of Medicine in Atlanta. As viruses spread, they can pick up genetic changes that help them adapt in ways that endanger people. “Should we really be waiting for a new variant to emerge before we, all of a sudden, are playing catch-up again with a public health emergency declaration to respond to [mpox], when we could have done that in [2022]?”
In the wake of the latest public health emergency declaration, countries including Japan, Spain and the United States are pledging vaccine donations to affected places. Meanwhile, nearly 6,000 mpox cases are confirmed in 15 African countries as of September 13, with tens of thousands more suspected, and 724 people have died. Here’s what we know so far about the latest mpox outbreaks and the viruses causing them, and what researchers still hope to learn.
What are clade I and clade II? How are they different?
When talking about viruses, “clade” refers to groups of close relatives that cluster together on the viral family tree. The viruses that cause mpox can be sorted into clade I and clade II; each circulate in different parts of Africa.
Historically, clade II viruses jumped from animals to people in parts of West Africa, including Sierra Leone and Nigeria. But around 2014, a clade II virus began spreading among people, researchers reported in a preprint posted June 19 at medRxiv.org that has yet to be peer reviewed. Public health officials first detected cases in humans in 2017. Five years later, in 2022, the outbreak went global, mostly spreading among sexual networks of men who have sex with men (SN: 7/22/22). Clade II viruses still circulate in Nigeria, and cause sporadic cases elsewhere.
Two groups of clade I viruses, called clade Ia and clade Ib, both usually found in Congo, are the focus of the new public health emergency. Clade Ia primarily affects children. That’s in part because kids like to play in forests, where they might come into contact with infected animals, Nachega says, though there is occasional transmission among people. In 2023 and 2024, clade Ia cases have also popped up in the Central African Republic and the Republic of Congo.
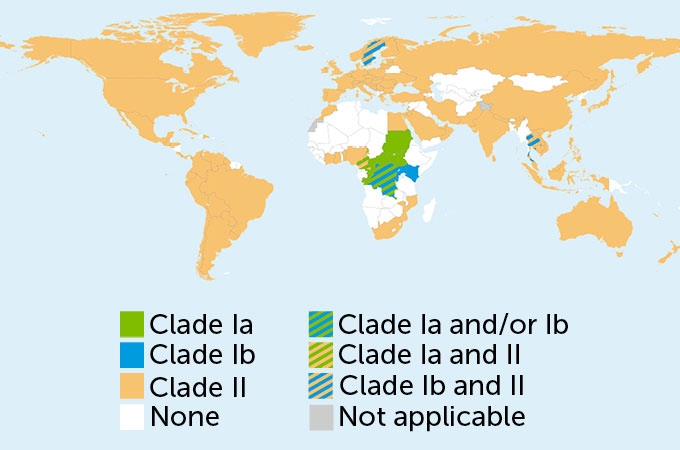
Global spread
Two groups of monkeypox viruses called clade I and clade II cause mpox. Each group is detected in different parts of the world. Two subgroups of clade I, named clade Ia (green) and clade Ib (blue), are mostly found in the Democratic Republic of Congo. Both have spread to neighboring countries and clade Ib has been detected in travelers to Sweden and Thailand. Clade II (orange) is mostly found in parts of West Africa. Following an outbreak in Nigeria, clade II viruses sparked international spread in 2022.
Mpox virus clades around the world, January 2022–September 2024
Then in September 2023, there was an mpox outbreak with human-to-human transmission in Kamituga, a mining area in eastern Congo. Like those caused by clade II viruses, the outbreak was linked to sexual contact, this time including sex workers and their clients. The new viral clade behind the outbreak, which Nachega and colleagues dubbed clade Ib, has mutations indicative of human-to-human transmission, the team reported June 13 in Nature Medicine. “It was the first scientific confirmation that something new happened with this virus,” Nachega says.
To date, clade Ib viruses have spread to four of Congo’s neighboring countries — Burundi, Kenya, Rwanda and Uganda — and some travel-related cases have popped up in Sweden and Thailand. Spread has also seemingly expanded beyond sexual networks to move through households, likely through close contact. In Burundi, around 30 percent of cases confirmed as of August 17 have been in children under 5 years old.
Clade I viruses may be more severe and deadly than clade II versions, according to the WHO. But the data are murky. Because the clades affect different populations, it’s possible that factors like age or quality of health care cloud the picture, making the disease seem deadlier in some places than in others.
Why is mpox spreading so widely now compared with previous outbreaks?
After the WHO declared smallpox, a closely related virus, eradicated in 1980 and ceased vaccinations, people have over time become more susceptible to mpox outbreaks. Now, with immunity that once protected against both viruses declining in Africa and around the globe, cases of mpox are on the rise.
But researchers have myriad questions about how specifically clade Ia and Ib viruses are spreading.
For instance, more than half of 5,000 confirmed mpox cases in Congo as of September 5 have been among children under the age of 15, according to the Africa Centres for Disease Control and Prevention. While clade Ib has hit adults hard, kids in this age group have faced worse outcomes than adults after getting infected with viruses from either clade. It’s unclear how many cases are in infants, young children or teenagers, and it’s possible that different activities are behind the virus’ spread in each group, Titanji says. Caregivers might expose young children through close contact as they carry infants in their arms. Older children may be exposed while working in mines and being in contact with other adults.
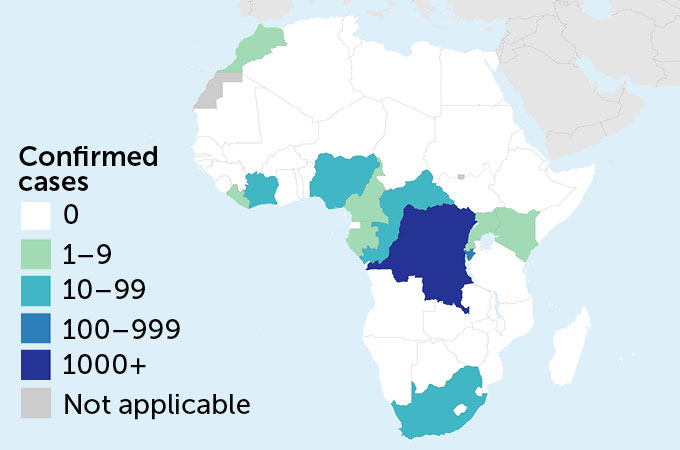
A new outbreak
In September 2023, clade Ib viruses sparked an outbreak of mpox in the Congolese mining town of Kamituga. Since January 2024, Congo has reported more than 6,500 confirmed cases of clade Ia and clade Ib mpox, with tens of thousands more suspected cases. The viruses have also spread to neighboring countries, including Burundi and Republic of Congo. Burundi and three other countries — Kenya, Rwanda and Uganda — have never reported mpox before.
Mpox cases in Africa, January–September 2024
Some transmission could be happening through respiratory droplets that get released through talking or breathing. Although most transmission happens through close contact, overcrowded households, where children come together with other family members, could offer the virus multiple routes to spread among many people.
“If you don’t understand these transmission dynamics, it makes it harder to predict” what could happen when the virus makes the jump to another country or continent where lifestyles differ, Titanji says. If there were an outbreak outside central Africa, for instance, “would we see a disproportionate impact on children?”
The virus is also spreading through sexual networks in adults, Titanji says. She’d like to know whether the virus hangs around in some parts of the body, making some forms of contact riskier than others, or whether people can transmit the virus to others even when they don’t have symptoms.
Are vaccines essential to control the virus’s spread?
Vaccines are among the best tools available. Africa CDC has said that the continent needs around 10 million vaccine doses to bring the mpox outbreaks under control. But given previous difficulties in getting shots in hand, and hurdles to manufacture enough doses, that is a tough bar to meet.
Also, “we still need hard data” to understand how effective existing smallpox vaccines are at protecting people from clade Ib viruses, Nachega says. Researchers are developing mpox-specific vaccines (though those aren’t yet ready to test in humans so aren’t useful in the current outbreak). One candidate outperformed the smallpox shot Jynneos at protecting rhesus macaques from mpox, researchers reported September 4 in Cell. Vaccinated animals had fewer lesions and fewer days of symptoms than those given either Jynneos or a placebo.
“We can’t have another vaccine-based strategy,” Ayoade Alakija, an infectious diseases physician and chair of the African Union’s Vaccine Delivery Alliance, said during an Aug. 28 briefing on mpox at the WHO Regional Committee for Africa Meeting. “We must do primary health care. We must do the basic things. It’s not just about vaccines.”

A handful of drugs exist to treat smallpox, for instance. But it’s unclear how effective those antivirals fare against mpox. A recent test of the drug tecovirimat showed that the rashes of treated people infected with clade I viruses didn’t resolve any faster than those given a placebo.
Helping people understand how to change behavior in ways that help curb transmission is also important, Titanji says. During the 2022 outbreak, activists lead the messaging that the virus that causes mpox was spreading among men who have sex with men, and that limiting sexual encounters could protect people from getting mpox. “And that worked,” Titanji says.
Still, without enough shots to protect high-risk groups in affected countries, the outbreak will probably continue for some time, Nachega says. “Nobody is safe until Africa is safe.”
#vaccines #mpox #reach #Africa #questions #remain #virus
Image Source : www.sciencenews.org